Laurie's Blogs.

Apr 2026
Utilizing Research on Degenerative Lumbosacral Stenosis in Dog to Formulate a Rehab Plan
Degenerative lumbosacral stenosis (DLSS) is a leading cause of caudal lumbar pain and cauda equina compression in middle-aged to geriatric large-breed dogs. It involves progressive degeneration of the L7-S1 intervertebral disc, ventral bulging of the ligamentum flavum, foraminal narrowing, and dynamic instability, leading to nerve root compression. Clinical presentation typically includes lumbosacral pain, hindlimb weakness or intermittent lameness, reduced jumping ability, crouched stance, and potential root signature signs.
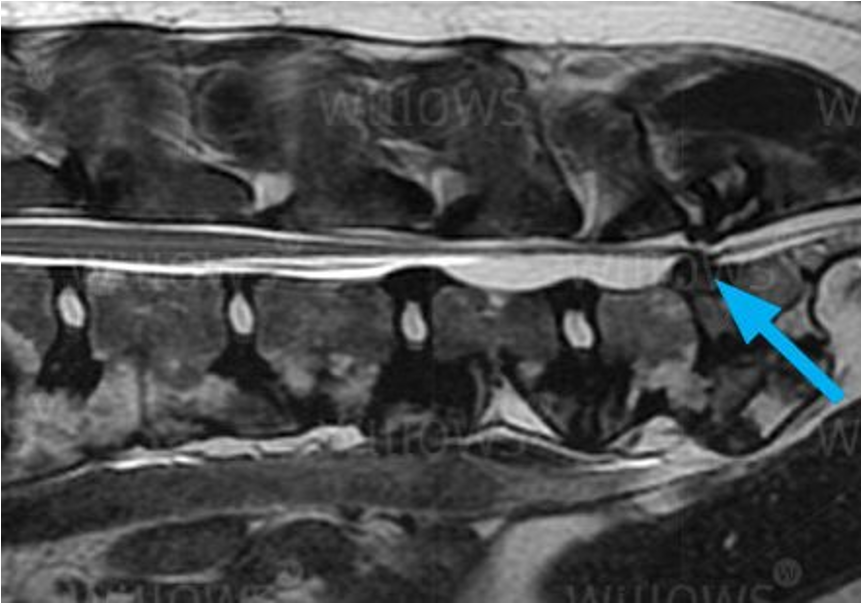
The 2026 retrospective study by Clemot et al. (Veterinary Surgery) evaluated dynamic MRI in neutral and flexed positions in 24 dogs with confirmed DLSS. Flexion produced significant reductions in intervertebral disc protrusion, protrusion ratios, ventral bulging of the ligamentum flavum, and foraminal compression (p < .001 for all), with complete resolution of cauda equina compression and foraminal occlusion in all cases. Improvement in disc protrusion correlated with the degree of disc degeneration (p = .004). These results suggest that flexion dynamically decompresses affected structures, supporting conservative approaches and questioning routine decompressive surgery when distraction-stabilization is planned.
How Can We Leverage This Study To Guide Rehabilitation?
Rehabilitation strategies can leverage these dynamic findings by incorporating flexion-biased techniques for decompression, followed by controlled progression to neutral spine stability and limited extension tolerance. The following revised exercise progression aligns with clinical principles of gradual loading, core activation, and avoidance of high-impact or excessive extension activities, which are contraindicated in DLSS due to exacerbation of compression.
Spinal Traction: Initial Mechanical Decompression
Traction remains a foundational intervention, providing controlled axial distraction to increase intervertebral space and reduce nerve root pressure, mirroring flexion-induced relief. Apply manual traction in sternal recumbency or supported standing, using low-grade (Grade I-II) sustained or oscillatory techniques for 30-60 seconds per cycle, repeated 3-5 times per session. Monitor for comfort and avoid extension bias. Integrate with initial rest (4-6 weeks of strict confinement with short leash walks for elimination) and multimodal pain control.
Mobilizations in Lumbar Flexion: Replicating Dynamic Relief
Passive and accessory joint mobilizations performed with the spine positioned in lumbar flexion directly exploit the study's demonstrated resolution of compression in flexed posture. Techniques include gentle oscillatory or sustained end-range flexion mobilizations at the L7-S1 segment, often combined with soft tissue release of paraspinal musculature and ligamentum flavum tension.
In clinical application, the dog is positioned over the therapist’s knee or thigh (depending upon size of the dog) or the therapists forearm under the dog’s abdomen encourages controlled flexion. Alternately the dog could be in lateral recumbency. From one of these positions, the therapist applying graded mobilization (i.e. transverse pressure on the spinous process, or a distraction between two spinous processes). These interventions aim to restore segmental mobility, reduce guarding in epaxial and iliopsoas muscles, and alleviate chronic nociceptive input. Manual therapy protocols emphasize starting with low-grade oscillations for pain-dominant presentations, progressing to higher-grade sustained holds as tissue tolerance improves. Such approaches align with multimodal conservative strategies, where flexion-biased mobilizations facilitate dynamic decompression without permanent surgical alteration of anatomy.
Progressive Core and Functional Exercises: Toward Neutral Stability
Following pain reduction and improved tolerance to flexion, transition to core activation and controlled loading in neutral spine alignment. Emphasize lumbopelvic control to support the degenerative segment without provoking extension-related compression. Progression should be individualized, slow (often over 8-12+ weeks), and supervised by a certified canine rehabilitation professional, with lifelong restrictions on high-impact activities (jumping, running off-lead, twisting).
Suggested progression:
• Pelvic tilt in sternal recumbency — Initiate core engagement with gentle anterior-posterior pelvic tilting in sternal position (down or supported prone). Use treat lures or light manual guidance to encourage subtle pelvic movement while maintaining neutral lumbar alignment, activating abdominals and deep stabilizers (multifidus equivalents). Perform 5-10 controlled repetitions, 2-3 sets daily, focusing on quality over quantity.
• Pelvic tilt in sitting — Advance to sternal-sitting transitions or supported sitting, cueing pelvic tilts to reinforce lumbopelvic dissociation and neutral posture control under partial weight-bearing.
• Stepping over low obstacles — Introduce controlled hindlimb proprioception and coordination with very low cavaletti rails or ground poles (e.g., 2-4 cm height). This promotes active pelvic control and hindlimb engagement without significant extension stress. Start with 5-10 passes, ensuring neutral spine maintenance.
• Controlled gradual extension loading — Only after consistent neutral stability, incorporate mild extension tolerance via walking up very gradual inclines (e.g., shallow hills or low ramps at <10°). Monitor closely for pain or compensatory patterns; limit to short durations and avoid steep grades.
• Front feet elevation with reach — Progress to placing front paws on a low step (e.g., 5-10 cm) while reaching upward for a treat, encouraging mild thoracic extension and core bracing while maintaining lumbosacral neutrality. This builds epaxial and abdominal endurance without full lumbar extension.
• Stair negotiation as functional assessment — Use ascending/descending low stairs (or equivalent ramps) as a late-stage test of integrated control and tolerance. This serves primarily as an outcome measure rather than a primary training exercise, performed sparingly to assess progress without risking flare-ups.
Throughout progression, prioritize low-impact activities, weight management, and avoidance of jumping, twisting, or high-speed play. Core-focused exercises aim to enhance neuromuscular control and reduce asymmetry, supporting long-term function within realistic limits. Dogs with DLSS typically achieve meaningful improvement in comfort and mobility but require permanent modification of high-impact behaviors to prevent recurrence.
Clinical Integration and Considerations
The dynamic MRI evidence bolsters flexion-based decompression in early rehab, transitioning to neutral stabilization for durability. Combine with pharmacotherapy (NSAIDs, gabapentinoids), weight optimization, and adjunct modalities as indicated. Prospective studies are needed to validate specific exercise protocols against surgical outcomes.
In practice, tailor interventions via serial assessments of pain, gait, neurologic status, and functional tolerance. Certified rehabilitation therapists should guide implementation to optimize safety and efficacy, enhancing quality of life while respecting the biomechanical realities of DLSS.
That’s it!
Until next time, Cheers!
Laurie
Reference:
Baldo Clemot I, Briola C, Ekiri AB, et al. Dynamic magnetic resonance imaging of the lumbosacral spine in neutral and flexed position for presurgical assessment of clinically affected dogs with degenerative lumbosacral stenosis. Veterinary Surgery. 2026; 55(1): 153-164.
